Look Up Facts
We are human and can make mistakes too. If you find something incorrect, feel free to point it out to us, and we will check it to see if your input is valid. We will not argue with any of you. Please provide factual evidence, not a narrative.
.
Two Distinct Definitions
The term "med beds" currently refers to two completely different things. One is a documented conspiracy theory involving fictional miracle-cure devices. The other is legitimate, advancing smart hospital bed technology. Both are addressed here.
The "Med Bed" Conspiracy Theory
Medbeds are a nonexistent medical technology that became prominent in conspiracy theory narratives in the early 2020s. These theories claim medbeds can supposedly cure any condition but have been kept secret from the general public and reserved for the elite.
Typical iterations describe three types, holographic diagnostic and curative, regenerative and limb-growing, and age-reversing, sometimes attributed to secret military programs or alien technology. No credible evidence of such devices exist.
The FDA has repeatedly warned companies marketing "med beds" or similar energy devices for unproven medical claims, and independent investigations by the BBC, AP, and Reuters consistently find zero measurable effects beyond placebo. Holistix Intl
On September 27, 2025, an AI-generated video styled as a breaking news clip from Fox News, claiming that a rollout of "MedBed hospitals" and "MedBed cards" was imminent, was posted to Donald Trump's account on Truth Social. Multiple outlets reported the clip was fabricated; Fox News stated that the segment had never aired on its network. The post was deleted the following morning.
No medbed device has any legitimate regulatory approval, because no real medbed has ever been demonstrated to work. The ones seen in online ads are either CGI renderings or repurposed health spa equipment. Perhaps the most tragic risk is that vulnerable people might delay or forgo real medical treatment because they are hanging their hopes on a medbed. PostQuantum
The idea that illness is due to "bad frequencies" and that putting "good frequencies" back inside the body will heal you is a common trope in a false alternative medicine, one which does not align with any human biology. Office for Science and Society
Real Smart Medical Bed Technology (2025)
This is where the legitimate science lives.
Smart beds are developed by integrating technology and communications, such as computer vision, artificial intelligence, machine learning, deep learning methods, and the IoT, for rapid and precise monitoring of patients.
These beds are equipped with a myriad of sensors and monitors that enable real-time monitoring of vital signs, including heart rate, blood pressure, respiratory rate, body temperature, and movements. Smart beds transmit clinical data wirelessly to healthcare providers, enabling them to closely monitor patients and provide immediate attention if any abnormalities are detected. News-Medical
Looking to the future, smart beds will likely evolve into platforms for automated drug delivery, voice-activated diagnostics, and advanced rehabilitation. AI-driven analytics can predict adverse events like sepsis or cardiac arrest based on subtle changes in collected data. Smart HealthCare
Embedded sensors capture vital signs such as heart rate, respiratory rate, and even subtle movement patterns like micro-shifts in weight or posture. The moment a patient's vitals deviate from normal thresholds, alerts are triggered, allowing for early intervention. It eliminates the lag between the onset of a complication and clinical response. Aslams
Smart hospital beds that use wireless sensor networks have led to a seamless and efficient solution to avoid bedsores in motion-impaired patients. Thrive by WHX
Futuristic concepts for multi-modality medical beds under research and development include red light therapy, magnetic resonance field therapy, hyperbaric oxygen therapy, nanotechnology integration, AI-driven diagnostics, soundwave therapy, and cryogenic micro-dosing.
Nanotechnology integration would theoretically deploy tiny biocompatible nanobots to target specific areas of the body, repairing tissues or delivering precise doses of medication. These remain largely speculative future concepts, not current deployments. WorldHealth
Citations
Abu-Zeinah, G., et al. (2025). Real-world analysis of polycythemia vera treatment reveals nonadherence to NCCN guidelines in a large proportion of patients. Blood Neoplasia, 2(4): 100167. https://ashpublications.org/bloodneoplasia/article/2/4/100167
Tan, G., et al. (2025). Improving the management of polycythemia vera patients eligible for cytoreduction. Taylor & Francis Online. https://www.tandfonline.com/doi/full/10.1080/03007995.2025.2458531
Hassanein, D. (2025). Advances in polycythemia vera treatment with targeted therapies and clinical trials. Discover Oncology / PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC12559549/
Tefferi, A. (2024). Polycythemia vera: 2024 update on diagnosis, risk-stratification, and management. American Journal of Hematology. https://pubmed.ncbi.nlm.nih.gov/37357958/
Tefferi, A., & Barbui, T. (2017). Polycythemia vera and essential thrombocythemia: 2021 update on diagnosis, risk-stratification and management. American Journal of Hematology. Referenced in: https://thepatientstory.com/mpn/polycythemia-vera/prognosis/
Tefferi, A., et al. (2013). Survival and prognosis among 1,545 patients with contemporary polycythemia vera: an international study. PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC3768558/
Griesshammer, M., Gisslinger, H., Mesa, R. (2015). Current and future treatment options for polycythemia vera. Annals of Hematology / PMC. https://pmc.ncbi.nlm.nih.gov/articles/PMC4420843/
Wikipedia. (Updated 2025). Polycythemia vera. https://en.wikipedia.org/wiki/Polycythemia_vera
Wikipedia. (Updated January 2026). Medbed. https://en.wikipedia.org/wiki/Medbed
McGill University, Office for Science and Society. (August 7, 2025). Med Beds: Not Today, Maybe Tomorrow? https://www.mcgill.ca/oss/article/medical-pseudoscience-technology/med-beds-not-today-maybe-tomorrow
Post Quantum. (October 1, 2025). Quantum MedBeds and Death Threats. https://postquantum.com/quantum-computing/quantum-medbeds/
News-Medical. (March 12, 2025). The Future of Hospital Care with Smart Bed Technology. https://www.news-medical.net/health/The-Future-of-Hospital-Care-Embracing-Smart-Bed-Technology.aspx
Smart HealthCare US. (April 3, 2025). Smart Beds and Patient Monitoring: The Future of In-Hospital Care. https://smarthealthcareus.com/2024/04/02/smart-beds-and-patient-monitoring-the-future-of-in-hospital-care/
WorldHealth.net. (March 31, 2025). Unveiling the Promise of Med Beds: The Potential Future of Healing. https://worldhealth.net/news/promise-of-med-beds-potential-future-healing/
Medical News Today. (March 12, 2024). Polycythemia vera diet FAQ. https://www.medicalnewstoday.com/articles/polycythemia-vera-diet-faq
Healthline. (February 27, 2024). Polycythemia vera self-care. https://www.healthline.com/health/polycythemia-vera/polycythemia-vera-self-care-from-head-to-toe
Experiments
We are human and can make mistakes too. If you find something incorrect, feel free to point it out to us, and we will check it to see if your input is valid. We will not argue with any of you. Please be able to provide factual evidence, not a narrative.
Understanding Memory Manipulation:
What You Need to Know
What You Need to Know
What Is Memory Manipulation?
Scientists have discovered ways to change, strengthen, or weaken memories in people's brains. This started with mouse experiments in 2013, where researchers could plant false memories directly into brain cells using light. Today, the technology is advancing toward human treatment.
How Does It Work?
The Basic Idea:
Memories are stored in specific brain cells.
Scientists can now:
Identify which brain cells hold a particular memory
Turn those cells on or off using light, electricity, or magnetic stimulation
Add new information while a memory is being recalled, changing how the memory gets stored
Strengthen fading memories or weaken painful ones
Three Main Technologies:
Optogenetics - Using light to activate specific brain cells
CRISPR gene editing - Modifying the genes in brain cells to make them respond to light
Deep brain stimulation - Using electrical implants to stimulate brain tissue
The Benefits
Medical Uses
- Alzheimer's disease - Restoring lost memories or slowing memory loss
- PTSD (Post-Traumatic Stress Disorder) - Reducing the emotional pain of traumatic memories without erasing them
- Phobias and anxiety - Weakening fear-based memories that cause ongoing panic
- Depression - Reactivating positive memories to help lift mood
- Addiction - Weakening cravings tied to drug-associated memories
Current Progress
Human trials are happening right now:
- A new Alzheimer's drug got FDA approval for human testing in 2025
- Researchers are enhancing memory consolidation (the process of turning short-term memories into long-term ones)
- Scientists are developing "memory prosthetics" - brain implants that could restore memory function
The Harms and Risks
Personal Identity Problems
When you change someone's memories, you change who they are. Memories make up our sense of self, our life story, our values. Altering them can:
- Disrupt your sense of who you are
- Disconnect you from your own experiences
- Damage your relationships if you no longer remember shared experiences the way others do
- Change how you feel about your own past actions
Ethical Issues
- Loss of authenticity - Your memories become what someone else programmed them to be, not what you actually experienced
- Moral responsibility - If memories of harmful actions are erased, the person may not feel accountability for what they did
- Social consequences - If people can forget injustices they've experienced, they may lose the motivation to fight for change or justice
Potential for Misuse
- Criminal justice - Defendants could erase memories of crimes they committed
- Political abuse - Governments could force memory alteration on prisoners or dissidents
- Corporate control - Companies could alter consumer memories to make them forget product defects or harmful practices
- Forced erasure - Involuntary memory alteration without consent
Military and Government Applications
How Governments Could Use This Technology
On Soldiers:
- Erase traumatic memories of killing, witnessing death, or committing atrocities, so soldiers don't develop PTSD or moral guilt
- Implant false memories making soldiers believe they were defending their country when they were actually committing war crimes
- Enhance loyalty by altering memories of orders or policies soldiers disagreed with
- Create super-soldiers who remember only success and forget failures, fear, or doubts
- Remove moral memory - alter memories of civilian casualties or ethical violations so soldiers don't question orders
On Prisoners or Political Detainees:
- Erase memories of torture so victims can't testify or have evidence of what happened
- Remove memories of resistance to weaken dissidents' commitment to their cause
- Implant confessions - make prisoners "remember" committing crimes they didn't actually commit
- Alter political beliefs by changing memories of key events or speeches that motivated opposition
- Create compliant citizens by erasing memories of government abuses or corruption
On Populations:
- Rewrite history by altering shared memories of major events (wars, massacres, government actions)
- Control narratives by making people forget inconvenient truths about government actions
- Suppress dissent by making people forget why they protested or what injustices motivated them
- Create false national memories to unite people around fabricated shared experiences or enemies
Real-World Concerns
Why This Is Dangerous Right Now:
- No international laws prevent governments from using this technology on their own citizens or prisoners
- Military funding - Governments are already funding neurotechnology research, including memory research
- Classified programs - Much neurotechnology research is classified, so we don't know what's actually being developed
- No enforcement mechanism - Even if laws existed, there's no way to verify a government isn't secretly using memory alteration
- Dual-use technology - The same tools designed to help PTSD patients can be weaponized against prisoners
Historical Parallels
This isn't purely theoretical. Governments have tried to control memory before:
- MK-Ultra program (1950s-1970s) - The CIA used drugs, hypnosis, and sensory deprivation to try to control minds and create amnesia
- Soviet Union - Political prisoners were forced into psychiatric institutions where their memories of dissent were "treated"
- Nazi Germany - Controlled information and propaganda to reshape how people remembered history
- China's Reeducation Camps - Use psychological techniques to alter beliefs and memories of detained populations
Memory manipulation technology would be far more effective than these crude methods.
The Soldier's Dilemma
Consider a real ethical problem:
A soldier experiences severe PTSD from combat. Memory dampening could help them sleep, reduce nightmares, and stop intrusive thoughts.
However, if the military uses this technology for other things, it could:
- Erase the soldier's memory of what actually happened, preventing them from testifying about war crimes
- Remove the soldier's moral awareness of their own actions
- Make it impossible for the soldier to hold their government accountable
- Create soldiers who feel no guilt about actions that should trigger moral reflection
The question: Is healing PTSD worth potentially erasing the moral memory that makes accountability possible?
Warning Signs to Watch For
- Government funding of memory manipulation research without public oversight
- Military applications described as "soldier wellness" or "trauma treatment"
- Classification of neurotechnology research as "national security"
- Laws passed that restrict your right to your own memories (forced memory alteration)
- AI systems used by law enforcement that could implant false memories in interrogations
- Neurotech devices sold to military or police without civilian review
False Memories from AI
Recent research (2024-2025) found that AI chatbots can accidentally or intentionally create false memories. In studies, people who chatted with AI about events they witnessed were more likely to "remember" things that never happened. Generative AI (like advanced chatbots) were especially effective at implanting false memories.
Current Safety Measures
What IS in place:
- FDA approval required for drugs used in clinical trials
- Institutional Review Boards (IRBs) review human studies
- Informed consent requirements - people must agree to participate
- Publication in peer-reviewed journals for scientific transparency
What IS NOT in place:
- No comprehensive oversight - There are no independent agencies specifically monitoring memory manipulation research
- No regulations - The FDA hasn't created specific rules defining what memory manipulation is ethical and what isn't
- No restrictions on context - There are no laws preventing use of memory technology in criminal justice, politics, or military settings
- No consumer protection - Direct-to-consumer neurotechnology products (brain-stimulation devices, apps, etc.) sold online have minimal oversight
- No clear rules for AI-generated false memories - No regulations govern how AI should be used in contexts where false memories could form
The Safeguards Scientists Say We Need (But Don't Have Yet)
Better consent processes
People need full, honest information about all risks before they participate
Clear legal boundaries
- Specific laws defining what uses are allowed and forbidden
- Restrictions on use in criminal justice, military, and politics
- Protections against forced memory alteration
Independent oversight boards
- Government agencies specifically dedicated to monitoring memory technologies
- Regular audits of how the technology is being used
- Power to stop research or products that pose serious risks
Protection from AI misuse
- Clear rules about when and how AI can interact with people's memories
- Requirements that people know they're talking to AI
- Safeguards to prevent accidental or intentional false memory creation
Bottom Line
Memory manipulation technology has genuine promise for helping people with Alzheimer's, PTSD, and other serious conditions. But it also has potential to be misused in ways that harm individual identity, justice, freedom, and society.
Right now, the technology is moving faster than the safeguards. We have therapeutic trials happening, but we don't have strong enough regulations to prevent abuse.
Key question for society: How do we gain the medical benefits while preventing the harms?
What Restrictions MUST Be Put in Place
Legal Protections Everyone Should Demand
1. Ban on Forced Memory Alteration
Memory manipulation should never be forced on anyone without their explicit, written, informed consent. This includes prisoners, soldiers, psychiatric patients, and children. Consent must be freely given—not coerced by threat of punishment or promise of reward. ANY violation should be a serious federal crime with prison time.
2. Transparency and Disclosure Requirements
Any government, military, or law enforcement use must be publicly reported. Researchers must disclose all funding sources—no classified or hidden memory research programs. Citizens have a right to know if their government is developing this technology. Companies selling neurotech devices must clearly disclose what they do and what they don't do.
3. Criminal Justice Protections
Memory evidence obtained through memory manipulation is inadmissible in court. Defendants have the right to know if anyone attempted to alter their memories. Prosecutors cannot use memory manipulation on witnesses or suspects. Police cannot use AI chatbots to implant false memories during interrogations. Any attempt to erase or alter a witness's memories is a federal crime.
4. Military and War Restrictions
Soldiers cannot be required to undergo memory alteration. Memory dampening for PTSD must be voluntary, with independent medical oversight. Memory alteration cannot be used to erase evidence of war crimes or atrocities. International law should prohibit memory manipulation as a weapon or interrogation tool. Soldiers retain the right to remember and testify about what they witnessed.
5. Prisoner Protections
Prisoners retain ownership of their memories—no forced alteration. Prison systems cannot use memory manipulation as punishment or rehabilitation. Torture victims and political prisoners have special protections. Any use of memory technology in custody requires court order and independent review.
6. Protection of Personal Identity
Laws must recognize memory as fundamental to personal identity and autonomy. Unauthorized alteration of memory is a violation of human rights. People have the legal right to their authentic memories, even if those memories are painful. Identity harm from memory alteration is compensable through lawsuits.
7. AI and Technology Safeguards
AI systems cannot be used to deliberately implant false memories. Any AI interaction about past events must disclose that the person is talking to AI. Companies cannot use AI to alter consumer memories about their products. Penalties for AI-induced false memories should match penalties for other forms of deception or fraud.
8. Government Accountability
Create an independent federal agency to oversee all memory manipulation research
This agency has power to:
Audit any research or military programs, shut down unauthorized programs, investigate and prosecute violations, and report regularly to Congress and the public. Whistleblower protections for anyone reporting illegal memory manipulation should also be included.
9. Medical Ethics Oversight
Institutional Review Boards (already exist) must have enhanced authority. Boards can reject any research that poses identity harm or misuse risk. Independent ethicists must review military and government applications. Patients have right to withdraw consent at any time.
10. International Cooperation
Treaty banning memory manipulation as a weapon (like biological weapons treaties), International inspections of neurotechnology research facilities, Enforcement mechanisms with real penalties for violations, and Protection for defectors or whistleblowers from other countries.
Why These Restrictions Matter
Without these protections:
Governments could create soldiers with no memory of atrocities
Regimes could erase dissidents' memories of oppression
Corporations could make people forget product defects that harmed them
Innocent people could be convicted based on false memories implanted by police
Whistleblowers could have their memories of corruption erased
Entire populations could have their history rewritten
With these restrictions:
Memory manipulation stays a medical tool, not a weapon
Individual rights are protected
Accountability for wrongdoing remains possible
Truth-telling is protected
Government power is limited
What Citizens Can Do Now
Demand transparency - Ask your representatives: Is your government funding memory research? What are the safeguards?
Support regulation - Back laws that protect memory as a fundamental right
Watch for warning signs - Notice if:
Military announces "trauma treatment" programs with classified budgets
New neurotech devices are sold without clear disclosure
Government research on neurotechnology is classified
Police or prosecutors start using AI in interrogations
Protect your rights
Know that memory alteration without consent should be illegal where you live
Spread awareness - Share information about this technology so people understand both benefits and dangers
Citations:
Tonegawa, S., et al. (2013). "Creating a False Memory in the Hippocampus." Science, 341(6144).
https://www.science.org/doi/10.1126/science.1239073
MIT News. "Neuroscientists plant false memories in the brain." (2013).
https://news.mit.edu/2013/neuroscientists-plant-false-memories-in-the-brain-0725
Centre for Addiction and Mental Health. "New drug shows promise in reversing memory loss for early Alzheimer's patients." ScienceDaily. (2025).
https://www.sciencedaily.com/releases/2025/02/250204141840.
\htm
Chan, S., Pataranutaporn, P., et al. (2024). "Conversational AI Powered by Large Language Models Amplifies False Memories in Witness Interviews." MIT Media Lab.
https://www.media.mit.edu/projects/ai-false-memories/overview/
González-Márquez, C. (2023). "Neuromodulation and memory: exploring ethical ramifications in memory modification treatment via implantable neurotechnologies." Frontiers in Psychology, 14(1282634).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10764565/
Yang, J. (2024). "Ethical issues in memory modification technology: a scoping review." Journal of Bioethical Inquiry.
https://www.researchgate.net/publication/385011639_
Ethical_Issues_in_Memory_Modification_Technology_A_Scoping
_Review
Neuroba. (2025). "Exploring the Ethical Implications of Memory Manipulation."
https://www.neuroba.com/post/exploring-the-ethical-implications-of-memory-manipulation-neuroba
Perelman School of Medicine, University of Pennsylvania. "Oversight of direct-to-consumer neurotechnologies: Efficacy of products is far from clear." (2019).
https://pmc.ncbi.nlm.nih.gov/articles/PMC6629579/
Annals of Abbasi Shaheed Hospital. "The Future of Neuronal Memory Manipulation: Therapeutic or Dangerous?" (2025).
https://www.annals-ashkmdc.org/index.php/ashkmdc/article/view/1130
Ryan, T.J., Roy, D.S., Pignatelli, M., Arons, A., & Tonegawa, S. (2015). "Engram cells retain memory under retrograde amnesia." Science, 348(6238).
https://www.sciencedaily.com/releases/2015/05/150528142815.
htm
Ramirez, S., Tonegawa, S., & Liu, X. (2014). "Identification and optogenetic manipulation of memory engrams in the hippocampus." Frontiers in Behavioral Neuroscience, 7:226.
https://www.frontiersin.org/journals/behavioral-neuroscience/articles/10.3389/fnbeh.2013.00226/full
The Transmitter: Neuroscience News and Perspectives. (2025). "The buzziest neuroscience papers of 2023, 2024."
https://www.thetransmitter.org/community/the-buzziest-neuroscience-papers-of-2023-2024/
Roeder, B.M., et al. (2024). "Developing a hippocampal neural prosthetic to facilitate human memory encoding and recall of stimulus features and categories." Frontiers in Computational Neuroscience, 18(1263311).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10881797/
Facts about Data Centers
We are human and can make mistakes too. If you find something incorrect, feel free to point it out to us, and we will check it to see if your input is valid. We will not argue with any of you. Please be able to provide factual evidence, not a narrative.
Public Information Fact Sheet · May 2026
Data Centers: What They Are, What They Do, and What It Costs Us
An honest, sourced overview of why data centers exist, how they benefit everyday life, and what their real resource demands mean for ordinary Americans.
What Is a Data Center?
A data center is a large building, sometimes the size of several football fields, filled with rows of computer servers, storage systems, and networking equipment. These facilities store, process, and transmit the data that powers nearly every digital service Americans use. The term "the cloud" is simply a friendly name for this physical infrastructure. There is nothing virtual about it. Somewhere, there is a building, using real electricity and real water, making it work.
There are currently approximately 11,800 data centers operating globally. More than 4,000 of them are located in the United States, representing 37% of the world's total. The rapid expansion of these facilities is driven primarily by the growth of artificial intelligence, but AI is far from their only purpose.
What Do They Actually Do for Us?
Every one of the following services depends on data centers operating continuously, around the clock:
🏥
Healthcare
Patient records, telemedicine visits, medical imaging, prescription routing, and emergency room data all run through data centers. Remote monitoring platforms for diabetic patients have been shown to reduce hospitalization risk by 18%. NHS digital programs integrating wearable data decreased emergency visits by 23% among patients with chronic conditions.
🚨
Emergency Services
Every 911 call is routed through data center infrastructure. Dispatch systems, police databases, fire department records, and FEMA emergency coordination all depend on these facilities being operational. A single large data center outage in 2025 triggered more than 6.5 million website disruptions, affecting banking, logistics, and government operations simultaneously.
🏦
Banking and Finance
Every ATM withdrawal, mobile deposit, credit card transaction, and wire transfer is processed through data centers. The global financial system has no offline alternative. When data centers go down, financial markets follow.
🗺️
Navigation and Weather
GPS navigation on your phone, real-time traffic updates, and weather forecasts all require data center processing. The International Energy Agency notes that AI running in data centers is now producing more accurate weather outlooks than previous forecasting methods.
🎓
Education
Online learning platforms, school administration systems, digital libraries, and remote classrooms all rely on data center infrastructure. During the COVID-19 pandemic, data centers made it possible for millions of students to continue their education without setting foot in a building.
🔬
Scientific Research
Drug development, protein mapping for disease treatment, climate modeling, seismic research, and cancer research all require the processing power that only data centers can provide. AI running in data centers is currently being used to rapidly map protein structures that would have taken years to analyze by hand.
🏛️
Government Services
Tax filing, voter registration, Social Security administration, passport issuance, driver's license processing, and public benefit management all run on government data centers. Smart city infrastructure, which manages traffic lights, public transit, and utility grids in real time, depends on them as well.
🛡️
National Security
Defense systems, intelligence operations, cybersecurity monitoring, and military communications all depend on secure data centers. Experts now describe data centers as the central nervous system of national infrastructure, comparable in strategic importance to what power plants were in the 20th century.
Why This Matters to Everyone
Data centers are not a technology product for tech companies. They are public infrastructure in the same practical sense as highways and power grids. When they work well and are managed responsibly, the benefits reach every household. When they are mismanaged, the costs reach every household too.
The Real Resource Costs — and What Is Being Done
1 Electricity: Does It Affect Your Bill?
The Impact
U.S. data centers consumed roughly 183 terawatt-hours of electricity in 2024, over 4% of all U.S. power use. That is approximately equal to Pakistan's entire annual electricity consumption. The Department of Energy projects data centers could account for 6.7% to 12% of all U.S. electricity by 2028.
Utilities requested more than $29 billion in rate increases in the first half of 2025 alone, which is double the amount from the year prior, with those costs passed to consumers. Electric bills rose approximately 10% nationally in 2025 compared to 2024. In some regions near data centers, electricity costs increased by as much as 267% compared to five years earlier.
What Is Being Done
A January 2026 Bloom Energy report projects total U.S. data center energy demand will nearly double between 2025 and 2028. In response, companies are moving toward solar, wind, nuclear, and geothermal power. Nuclear and geothermal provide the constant baseload these facilities require without the intermittency of renewables.
The U.S. Department of Energy has invested $40 million into liquid cooling research, which uses significantly less energy than traditional air cooling. Congress included a study in the FY2026 Energy and Water Appropriations Act to examine the impact of data center demand on residential utility bills and identify solutions. Amazon's independent rate study found that in some regions, data centers actually pay more than the cost of their electricity use, creating a financial surplus utilities can direct toward grid modernization.
The honest picture: Whether data centers raise your electricity bill depends heavily on where you live, how your state regulates utility rates, and whether your utility has introduced tiered pricing for large industrial customers to separate their costs from residential customers. The impact is real in some regions and minimal in others. Congress is actively examining this, and some states are already acting to protect residential ratepayers.
2 Water: Does It Affect Your Supply?
The Impact
Server stacks generate enormous heat, and the most common cooling method is evaporative cooling, which consumes large amounts of freshwater. U.S. data centers directly consumed 17.4 billion gallons of water in 2023. Google's data center water use rose from 4.3 billion gallons in 2021 to 6.1 billion gallons in 2024. A study by the Houston Advanced Research Center found Texas data centers could use up to 399 billion gallons of water annually by 2030.
Water returned to the supply carries higher concentrations of dissolved solids such as calcium, chloride, and silica, which can affect drinking water taste, reduce crop yields, and prove toxic to aquatic life.
What Is Being Done
Microsoft announced in December 2024 that all new data center designs from August 2024 onward use zero-water evaporation cooling technology, with pilot facilities in Phoenix and Wisconsin coming online in late 2027. The World Economic Forum's Nature
Positive Transitions initiative is working with technology companies to reduce water and energy impacts. Researchers from Diaz-Marin and Berquist published findings in 2025 in Energy and Environmental Science showing that with advanced cooling and intelligent heat management, data centers could theoretically capture carbon and produce water rather than consuming it. Some regions now legally require the use of gray or recycled water rather than freshwater for cooling.
The honest picture: For most Americans, data center water use does not directly affect what comes out of their tap today. The risk is concentrated in water-scarce regions, particularly in the Southwest and parts of Texas, where large-scale freshwater consumption competes with agricultural, municipal, and residential needs. The concern is legitimate, and the solutions are actively under development, though widespread adoption of zero-water cooling is still several years away.
Key Numbers
11,800 Global Data Centers
37% are in the U.S.
183 TWh U.S. Power Used (2024)
Equal to all of Pakistan's annual electricity
17.4B Gallons of Water (U.S., 2023)
Consumed directly in a single year
~10% Average U.S. Electric Bill Increase
2025 vs. 2024 Nationally
What We Do Not Yet Know
Research published in AGU Advances in February 2026 notes that few data center operators release data on individual facility consumption. Researchers describe the lack of transparency as a significant obstacle to accurate environmental assessment. A Harvard School of Public Health study from May 2025 identified data center health impacts as a largely overlooked area requiring urgent empirical research. When a growing piece of national infrastructure does not report its resource use publicly, independent verification is not possible.
The complete picture: Data centers are not the enemy of everyday Americans, and they are not consequence-free either. They power services that save lives, protect savings, educate children, and keep critical infrastructure running. They also consume electricity and water at a scale that has measurable effects on utility bills and, in some regions, on water availability.
The question worth asking is not whether data centers should exist. That we don't have a choice in. The question is whether the companies that profit from them are being held accountable for the real costs they create, whether those costs are being passed to ordinary households or absorbed by the industry, and whether the solutions now under development are being adopted at the pace the growth demands.
An informed public is better positioned to ask those questions of both elected officials and the technology companies themselves.
The Solutions
Full Paper and diagrams
PUBLIC DOMAIN, CC0 1.0 Universal
This work is released into the public domain under CC0 1.0 Universal.
No rights reserved. Copy it, build it, improve it, sell it, share it, translate it, freely, without restriction, without asking my permission. I give it out of the kindness of my heart, simply because I care about all people.
This framework was shared freely because people matter more than profit.
CC0 license: https://creativecommons.org/publicdomain/zero/1.0/
THE NET-POSITIVE DATA CENTER
A Solar-Powered, Gravity-Fed Closed-Loop Framework
for Cooling, Self-Sustaining Recirculation, and Net-Positive Grid Contribution
Originally conceived and shared freely by
https://mylearningacademy.org/realfacts/lookupfacts1.html | Creator of the Symbiotic Workforce
June 2026
A Note on This Document
This framework was developed and released freely into the public domain because the problems it addresses such as water shortages and grid strain caused by data center growth, are harming real people in real communities right now. No patent has been filed. No license fee will ever be charged. No permission is required to use, build, improve, or distribute any part of this work.
Every objection has already been answered:
"It costs too much" - Every component is already manufactured and deployed in other industries. No research and development required.
"It hasn't been proven" - Each component has decades or centuries of documented real world performance with citations to back every claim.
"We need the data centers for economic development" - The framework does not oppose data centers. It makes them better neighbors.
"The technology isn't ready" - It is not only ready, it is already running in multiple industries simultaneously.
"It will take too long to implement" - The phased deployment pathway means benefits begin accruing from phase one before the full system is even complete.
"It will hurt the data center operators financially" - Net metering revenue, eliminated water costs, and reduced grid draw actually improve the facility's operating economics.
"Communities won't see benefits fast enough" - Returns are immediate and measurable on the first utility billing cycle.
"It only solves one problem" - It solves water consumption, electricity drain, grid strain, noise pollution, community electricity costs, and drought vulnerability simultaneously.
If you are an engineer, a city planner, a utility operator, a developer, or a student who can make any part of this real, please do. The only goal is that people are harmed less. Everything else is secondary.
Executive Summary
Data centers have become the backbone of the modern digital economy. They also represent one of the fastest-growing simultaneous drains on two things cities cannot afford to lose: their electrical grid capacity and their municipal water supply. The current trajectory is not merely unsustainable in multiple regions of the United States, it is already in direct conflict with the basic needs of residential communities.
A solution exists that does not slow digital growth. It reverses the equation entirely. This paper proposes a closed-loop system that uses solar power to initially elevate water or a coolant fluid into a reservoir positioned directly above the data center. From that point forward, the system sustains its own operation through gravity-fed flow, thermosiphon convection driven by server heat, an overshot water wheel coupled to an alternator, and a hydraulic ram pump powered entirely by water pressure. The solar array, connected to the grid through net metering, generates surplus power that feeds back to the surrounding community. The facility stops pulling from the city. Instead, it gives back to the people it serves.
The Problem Part One: The Electrical Grid Cannot Keep Up
U.S. data centers consumed 176 TWh of electricity in 2023, representing 4.4% of total national electricity consumption. By 2024 that figure had climbed to 183 TWh. The U.S. Department of Energy projects this will rise to between 325 and 580 TWh by 2028, potentially reaching 12% of all U.S. electricity within that window.
Globally, data centers consumed approximately 415 TWh in 2024, about 1.5% of all electricity worldwide, and are projected to nearly double to 945 TWh by 2030, growing at roughly 15% per year, more than four times the growth rate of every other electricity sector combined.
In the 12 months ending November 2025, nearly 90% of the net change in installed U.S. generation capacity came from solar and batteries. Gas plants added just over 4 GW and delivery times are extending into the next decade with skyrocketing costs. Solar-plus-storage is the only generation capacity realistically available in the near term to meet rising data center demand. That reality makes on-site solar generation not an option but a structural necessity.
Cooling systems alone account for 30 to 40% of a data center's total energy use. The average Power Usage Effectiveness rating industry-wide is 1.56, meaning that for every unit of energy used on computing, an additional 56% is burned just keeping the machines cool.
The Problem Part Two: Cities Do Not Have a Steady Water Supply to Give
This section states the situation plainly because the data demands plain language. Data centers are not drawing from an inexhaustible resource. They are drawing from the same municipal water systems that communities depend on for drinking, sanitation, agriculture, and fire response, and those systems are already under a strain that is accelerating.
In 2023, U.S. data centers directly consumed 17.4 billion gallons of water. That figure is projected to rise to between 38 and 73 billion gallons by 2028, according to the EPA. Large data centers can use up to 5 million gallons of water in a single day, equivalent to the daily water use of a town of 10,000 to 50,000 people. In 2021, the nation's data centers collectively consumed an estimated 449 million gallons per day, totaling 163.7 billion gallons annually.
These numbers are not abstract. In Bessemer, Alabama, community opposition temporarily halted construction of a data center projected to require 2 million gallons of water per day, roughly enough to supply two-thirds of that city's population. Google's data center cluster in Dalles, Oregon, a city of 16,000, consumed 355 million gallons in 2021 alone, roughly a quarter of the city's total water use that year. The city initially refused to disclose this figure, citing it as a trade secret, and it took multi-year litigation to make the data public.
In Texas, data centers consumed over 50 billion gallons of water in 2024. A study by the Houston Advanced Research Center projected Texas data centers will use as much as 399 billion gallons by 2030, equivalent to drawing down Lake Mead, the largest reservoir in the country, by more than 16 feet in a single year. Texas is already in crisis: reservoirs and groundwater are drying up statewide, and Corpus Christi was preparing to declare a water emergency with mandatory 25% usage cuts.
In Arizona, municipalities in the Phoenix and Tucson regions face a critical threat from the looming shortage on the Colorado River. In the worst-case scenarios, the federal Department of the Interior could cut almost all water deliveries from the canal serving central Arizona. The Tucson City Council unanimously rejected a major data center project in August 2025, citing water concerns. Meanwhile, data center expansion continues at scale in the same drought-stressed region.
Roughly 80% of the water withdrawn by data centers evaporates. Industrial water-supply contracts negotiated with data centers typically include reservation provisions that protect industrial supply ahead of residential restrictions during drought. When a city enacts mandatory water cuts for its residents, the data center next door may be contractually protected from those same cuts.
The city does not have a steady supply of water to give. In multiple U.S. regions, that is the present reality, not a future projection.
The Solution: A Solar-Powered, Self-Sustaining Closed-Loop System
Core Concept
The proposed system addresses both the electricity problem and the water problem simultaneously. Solar panels power the initial elevation of fluid into a sealed elevated reservoir positioned directly above the data center. From that point forward, gravity, server heat, and water pressure sustain the system's own operation. The solar array generates more electricity than the facility's internal systems consume, and that surplus feeds back into the municipal grid.
The fluid loop is completely sealed, no municipal water is consumed, no water is discharged, and no water evaporates. Additinally, the city receives electricity from the facility. The city loses no water to the facility. That is the definition of net positive.
The Tree Principle: Thermosiphon Self-Reinforcement
Consider how a tree functions. Water drawn up from the roots does not require a mechanical pump. Heat from the sun causes moisture to evaporate from the leaves, creating a pressure differential that pulls water upward continuously. The thermal difference between the warm canopy and the cool root zone drives the entire system without external energy input.
The same principle, known in engineering as a thermosiphon, governs the self-reinforcing behavior of this data center cooling design. When fluid absorbs heat from the server racks, it becomes less dense and rises naturally toward the elevated condenser zone above, releases thermal energy, becomes denser, and descends. This cycle circulates the fluid continuously without mechanical assistance, as long as the thermal differential is maintained. Positioned directly above the heat source, the elevated reservoir and cooling loop form a vertical axis of thermal and gravitational force. The heat the servers generate is precisely what keeps the fluid moving.
The Water Wheel: Mechanical Energy Recovery
As the cooled, dense fluid descends from the elevated reservoir, it passes through an overshot water wheel, the same technology that powered farms and mills for centuries, now applied to one of the most urgent infrastructure challenges of our time.
An overshot wheel receives flow at the top, gravity fills its buckets, and it rotates under the weight of the descending fluid. Research published in the journal Renewable Energy confirmed that overshot water wheel designs achieve efficiencies of up to 85 to 90%. The wheel couples directly to an alternator, converting rotation into electricity. The wheel's axle simultaneously provides mechanical recirculation assist, recovering more energy from the descent than is needed to return a portion of the fluid to the elevated reservoir.
The Hydraulic Ram Pump: Self-Powered Recirculation
A hydraulic ram pump uses the pressure and momentum of flowing fluid to push a portion of that same fluid uphill with no external power source. It operates on the principle of water hammer: fluid builds momentum, a waste valve slams shut creating a pressure spike, and that spike forces a portion of the fluid back up into the elevated reservoir. Only two moving parts are needed.
Continuous automatic cycling and No electricity required::
A minimum head pressure drop of approximately 3 feet is all that is needed, easily met by any building elevation differential.
During peak computational activity, thermosiphon convection is strongest, fluid flow is fastest, and both the ram pump and water wheel perform at their highest output. Peak demand strengthens rather than strains the system.
Solar Connection: From Self-Sufficient to Net Positive for the City
This is the layer that transforms the system from self-sufficient to city-beneficial. The solar array, connected to the grid through net metering, generates surplus electricity that flows outward to the surrounding community during daylight hours, particularly when the thermosiphon and ram pump are handling recirculation without solar pump assistance.
Net metering is a billing mechanism that credits facility operators for the electricity they add to the grid. The Solar Energy Industries Association confirms that net metering policies exist in 34 states plus Washington D.C. and Puerto Rico, and that net metering creates a smoother demand curve for utilities while reducing peak load pressure on the grid.
Today, data centers are the reason neighboring residents face rising electricity rates, grid strain, and in some cases water shortages that affect household pressure and supply. Under this framework, the data center becomes the reason those same residents have lower electricity bills, a more stable grid, and no competition for their water. That is not just a minor improvement. It is a reversal of the relationship between digital infrastructure and the communities that host it.
Optional Coolant Enhancement: Glycol-Based Fluid
Automotive cooling systems use glycol-based antifreeze to keep engines operating at stable temperatures across a wider range of conditions than plain water alone. The same logic applies directly to this data center system, and it is already the industry standard at hyperscale facilities.
Glycol-based coolants, specifically propylene glycol or ethylene glycol mixed with water, are in active documented use in data center liquid cooling systems today. The industry standard for server-level cooling loops is a propylene glycol-water mixture at 30 to 50% concentration. Propylene glycol is preferred at the server level because it is non-toxic: a leak inside a GPU rack containing propylene glycol is far less hazardous than one containing ethylene glycol. In a sealed closed-loop system, the coolant circulates without escaping, just as antifreeze stays within a car's sealed cooling system.
Glycol adds four specific protections: freeze protection (a 50% ethylene glycol solution freezes at approximately -36 degrees Celsius, protecting outdoor and rooftop components in cold climates), corrosion inhibition (protecting copper, aluminum, and steel piping from electrochemical degradation), biocide function (resisting microbial growth that fouls heat exchangers), and thermal stability across seasonal variation.
The honest tradeoff must also be stated. Pure water has higher specific heat capacity, higher thermal conductivity, and lower viscosity than any glycol mixture, meaning it absorbs more heat per unit volume, transfers it more efficiently, and requires less pump energy to move. Glycol mixtures require larger flow channels or increased heat exchanger surface area to match water-only cooling performance at the chip level. Concentrations above 60% reduce performance due to increased viscosity.
This design recommendation is a dual-loop architecture the industry has already independently adopted in certain areas. The primary outdoor loop uses a glycol-water mixture for freeze and corrosion protection. The secondary server loop uses propylene glycol-water at lower concentration or carefully conditioned water in order to maximize heat absorption at the hardware level. A coolant distribution unit separates these loops via a heat exchanger, maintaining independent fluid chemistry in each. This architecture is documented in both the Open Compute Project guidelines and ASHRAE's TC9.9 technical bulletin on liquid cooling deployments.
The Elevation-Power Relationship
The degree to which a facility achieves net-positive status scales directly with the elevation differential between the reservoir and the water wheel. Power output equals water density multiplied by the acceleration of gravity, multiplied by flow rate, multiplied by head height. Greater elevation means greater pressure, faster flow velocity, and greater output per unit of fluid through both the alternator and the ram pump.
Height is not an aesthetic choice in this design. It is the primary engineering variable that determines how far above net-zero the facility operates. Purpose-built towers or elevated structural frames positioned directly above the facility can achieve elevation differentials well beyond standard rooftop placement.
System Components
• Solar Array: Roof-mounted or adjacent photovoltaic panels sized for surplus grid export via net metering. Provides initial reservoir charging. During steady-state operation, the thermosiphon, ram pump, and water wheel carry the recirculation load, freeing solar output for community contribution.
• Elevated Reservoir: Sealed, insulated tank positioned directly above the data center. Vertical alignment above the heat source ensures thermosiphon convection, gravitational head pressure, and ram pump drive pressure all act along the same vertical axis.
• Primary Outdoor Loop (Glycol-Water): Circulates between the elevated reservoir, external condenser, and coolant distribution unit. Uses inhibited glycol-water mixture for freeze and corrosion protection of exposed components.
• Secondary Server Loop (Propylene Glycol-Water or Conditioned Water): Circulates through server cooling manifolds. Uses propylene glycol-water or conditioned water to maximize heat absorption at the chip level while protecting hardware.
• Coolant Distribution Unit (CDU): Separates the two loops via heat exchanger. Transfers thermal energy between fluids without mixing them.
• Thermosiphon Circuit: Sealed piping allowing heated fluid to rise by convection toward the condenser above and cooled fluid to descend, without pump energy.
• Overshot Water Wheel with Coupled Alternator: Receives descending flow at the top, rotates under the weight of the fluid, drives the alternator to generate electricity, and provides mechanical recirculation assist via the axle.
• Hydraulic Ram Pump: Uses water hammer pressure from the falling flow to return a continuous portion of fluid to the elevated reservoir with zero electrical input. Requires only a minimum 3-foot head pressure drop.
• Net Metering Grid Connection: Bi-directional meter connecting the facility's solar and water wheel generation to the municipal grid. Surplus electricity flows outward to neighboring consumers.
• Battery or Capacitor Buffer: Modest storage bridging nighttime and overcast periods. Alternator output during operational hours supplements or replaces this draw.
How the Energy Math Works
The system combines five validated, independently deployed technologies: pumped storage hydropower (88% of U.S. utility-scale energy storage), thermosiphon passive cooling (no electrical input), overshot water wheel generation (up to 85-90% efficiency), hydraulic ram self-pumping (zero electrical input), and grid-connected solar with net metering (deployed in 34 states).
The cooling function, conventionally 30 to 40% of total facility energy, is performed without grid draw. The thermal energy that would otherwise be wasted becomes the driver of fluid circulation. The water wheel captures the energy of the descent. The ram pump closes the loop without external input. The solar array generates more than the remaining facility load. The net result flows outward to the city.
Because the thermosiphon and ram pump handle recirculation during operational hours without drawing from the solar array, a larger portion of solar output is available for grid export than in a conventional solar-supplemented facility. The closed fluid loop eliminates municipal water consumption entirely. The facility's contribution to the city is both electrical and hydrological.
Key Advantages of This Framework
Net Positive for the City, Not Just Net Zero for the Facility
Net zero means a facility neither takes from nor gives to the city. Net positive means the city receives more than the facility takes. This framework targets net positive in both electricity, through solar export via net metering, and water, through a completely sealed loop that draws nothing from municipal supply. That outcome is not achievable under any conventional data center design.
Mechanically Self-Sustaining
Thermosiphon convection, water wheel recirculation assist, and hydraulic ram pump return sustain the fluid cycle without continuous electrical input, freeing the majority of solar output for grid contribution rather than internal consumption.
Zero Municipal Water Consumption
The completely sealed closed loop retains every unit of fluid in the system indefinitely. No municipal water is consumed. No water is discharged. No water evaporates. In drought-stressed regions, which now include Texas, Arizona, Georgia, and large parts of the American West, this is the difference between a facility a city can permit and one it cannot afford to host.
Grid Contribution
Surplus electricity from the water wheel alternator and solar array feeds back to the municipal grid through net metering, reducing pressure on surrounding residential and commercial consumers. Each facility becomes a distributed generation asset rather than a grid liability.
Demand-Reinforced Performance
Higher computational demand produces more server heat, which strengthens thermosiphon convection, accelerates fluid flow, increases water wheel output, and improves ram pump efficiency. Peak demand is the condition under which this system performs best, the inverse of every conventional data center cooling architecture.
Implementation Pathway
New Construction
Facilities designed for this system should optimize for maximum vertical alignment: elevated reservoir directly above the server floor, straight vertical circuit, water wheel and ram pump in the descending flow path, dual-loop glycol architecture with CDU, and solar array sized for surplus grid export. Purpose-built structural towers achieve elevation differentials of 30 meters or more.
Retrofit of Existing Facilities
Existing data centers can retrofit by adding an elevated tower reservoir directly above the structure, installing closed-loop thermosiphon piping, positioning the water wheel and alternator in the descending circuit, adding the hydraulic ram pump in the lower collection section, converting the outdoor primary loop to glycol-water with CDU separation, and connecting an expanded solar array to the grid via net metering.
Phased Deployment
Phase one establishes the closed-loop thermosiphon cooling circuit and sealed fluid loop, immediately eliminating municipal water consumption and cooling-related grid draw. Phase two adds the elevated reservoir and water wheel alternator. Phase three integrates the hydraulic ram pump, achieving self-sustaining recirculation. Phase four converts the outdoor primary loop to glycol-water with CDU separation. Phase five connects an expanded solar array to the grid via net metering, completing the net-positive architecture.
Permitting and Policy Alignment
Cities considering data center development agreements have grounds to require this framework as a condition of permitting. A facility operating under this framework imposes no water cost on the city and contributes to grid stability rather than straining it. The policy case for requiring it is straightforward.
Broader Context: Why This Matters Now
The water situation is moving faster than most public reporting reflects. In Texas alone, the trajectory runs from 50 billion gallons consumed in 2024 to a projected 399 billion gallons by 2030, an eight-fold increase in six years, in a state where major reservoirs are already at historic lows. The Tucson City Council unanimously rejected a major data center project in August 2025, citing water concerns. Community groups in Georgia, Iowa, and Alabama have filed legal challenges and forced regulatory reviews based on water consumption projections.
This is not a future problem. It is an active civic conflict in multiple states simultaneously.
The hydraulic ram pump has been in documented use for over 200 years. Water wheels powered industrial civilization for centuries. Thermosiphon cooling is deployed today across dozens of industries. Glycol-based closed-loop cooling is the current industry standard at hyperscale facilities. Solar net metering exists in 34 states. None of this requires new invention. It requires integration and the will to build it.
Full Paper and diagrams
Conclusion
The data center industry is on a trajectory that, if unchanged, will drain municipal water supplies in dozens of U.S. cities and force communities to choose between hosting digital infrastructure and retaining access to their own water and electricity. In some regions, that choice is no longer hypothetical.
The framework in this document offers a complete alternative. The facility uses server heat to drive fluid circulation, uses falling fluid to generate electricity, uses that fluid's pressure to return itself to the elevated reservoir, uses glycol to protect outdoor components, and uses a solar array connected to net metering to give surplus power back to the homes and businesses around it. The closed loop draws nothing from the city's water system. The grid connection gives electricity to the city rather than taking from it.
This was shared freely because the people in those communities matter. Build it, improve it and share it further. No permission needed.
Full Paper and diagrams
Citations and Sources
All factual claims in this paper are drawn from the following primary and secondary sources. No data has been fabricated. Where projections differ between sources, the most conservative credible estimate is used in the body text.
1. Lawrence Berkeley National Laboratory (2024). 2024 United States Data Center Energy Usage Report. U.S. DOE. https://eta-publications.lbl.gov/sites/default/files/2024-12/lbnl-2024-united-states-data-center-energy-usage-report_1.pdf, Source for: 176 TWh in 2023 (4.4% of U.S. electricity); projected 325-580 TWh by 2028; 17 billion gallons water consumed 2023.
2. U.S. Department of Energy (2024). DOE Releases New Report Evaluating Increase in Electricity Demand from Data Centers. https://www.energy.gov/articles/doe-releases-new-report-evaluating-increase-electricity-demand-data-centers, Source for: Projected 6.7-12% of total U.S. electricity by 2028.
3. Pew Research Center (October 2025). US data centers' energy use amid the artificial intelligence boom. https://www.pewresearch.org/short-reads/2025/10/24/what-we-know-about-energy-use-at-us-data-centers-amid-the-ai-boom/, Source for: 183 TWh in 2024; projected 426 TWh by 2030; AI hyperscalers equivalent to 100,000 households; natural gas supplying 40%+ of data center electricity.
4. International Energy Agency (IEA, 2024). Energy demand from AI. https://www.iea.org/reports/energy-and-ai/energy-demand-from-ai, Source for: 415 TWh globally in 2024; projected 945 TWh by 2030; accelerated server consumption growing 30% annually.
5. Energy Institute Blog / UC Berkeley (March 2026). A Solution for the Fast Data Center Connection Challenge. https://energyathaas.wordpress.com/2026/02/02/a-solution-for-the-fast-data-center-connection-challenge/, Source for: 90% of net change in U.S. installed generation capacity in 12 months ending November 2025 coming from solar and batteries; solar-plus-storage as the only realistically available near-term capacity.
6. Fortune (May 2026). America's data centers are thirsty. Rural towns are paying the price. https://fortune.com/2026/05/13/data-center-georgia-arizona-water-wars/, Source for: 17.4 billion gallons consumed in 2023, projected 38-73 billion gallons by 2028 per EPA; Texas data centers projected at 399 billion gallons by 2030; Corpus Christi preparing water emergency with 25% mandatory cuts; Google's The Dalles facility consuming 355 million gallons in 2021.
7. Newsweek (May 2026). Map Shows Where Data Centers Are Being Built in Drought-Hit Areas. https://www.newsweek.com/map-data-centers-built-drought-hit-areas-11997520, Source for: Large data centers using up to 5 million gallons per day; Bessemer Alabama data center projected at 2 million gallons per day; industrial water contracts including reservation provisions protecting supply ahead of residential restrictions during drought.
8. Grist (March 2026). Arizona's water is drying up. That won't stop its data center rush. https://grist.org/technology/arizona-water-data-centers-semiconducters/, Source for: Colorado River shortage threatening central Arizona water deliveries; Tucson City Council unanimously rejecting Amazon-linked Project Blue data center in August 2025.
9. WaterVerge (May 2026). Data Centers Are Drinking Your Water. https://www.waterverge.com/news/data-centers-ai-water-consumption-2026/, Source for: Maricopa County data centers consuming 905 million gallons in 2025; industrial reservation provisions protecting data center supply during drought.
10. datacenters.com (July 2025). How Data Centers Are Shaping Texas's Water Crisis. https://www.datacenters.com/news/texas-water-crisis-the-impact-of-data-center-developments-on-a-fragile-resource, Source for: Texas data centers consuming over 50 billion gallons in 2024; Lake Travis, Lake Buchanan at historic lows; Edwards Aquifer 20 feet below 10-year average.
11. Solar Energy Industries Association (SEIA, 2024). Net Metering. https://seia.org/net-metering/, Source for: Net metering available in 34 states plus D.C. and Puerto Rico; net metering creating smoother demand curve and allowing utilities to better manage peak loads.
12. U.S. Department of Energy. Pumped Storage Hydropower. https://www.energy.gov/cmei/water/pumped-storage-hydropower, Source for: PSH accounting for 88% of all utility-scale energy storage in the United States.
13. DOE Technology Strategy Assessment (2023). Pumped Storage Hydropower. https://www.energy.gov/sites/default/files/2023-07/Technology%20Strategy%20Assessment%20-%20Pumped%20Storage%20Hydropower_0.pdf, Source for: Round-trip efficiency of new PSH plants at approximately 80%.
14. Quaranta, E. and Revelli, R. (2015). Output power and power losses estimation for an overshot water wheel. Renewable Energy, Elsevier, vol. 83(C). https://www.sciencedirect.com/science/article/abs/pii/S096014811500395X, Source for: Maximum efficiency of overshot water wheels at 85-90%.
15. Quaranta, E. and Revelli, R. (2018). Gravity water wheels as a micro hydropower energy source: A review. ScienceDirect. https://www.sciencedirect.com/science/article/pii/S1364032118306178, Source for: Overshot design achieving highest efficiency at lowest flow rates; modern designs maintaining high efficiency across wide range of conditions.
16. Water Center at Penn. Water-to-wire Micro-hydropower generation. https://watercenter.sas.upenn.edu/splash/water-wire-micro-hydropower-generation, Source for: Five components of an in-stream micro-hydro system including waterwheel, alternator, charge controller, and battery.
17. Hackaday (October 2025). How Hydraulic Ram Pumps Push Water Uphill With No External Power Input. https://hackaday.com/2025/10/02/how-hydraulic-ram-pumps-push-water-uphill-with-no-external-power-input/, Source for: Ram pump converting kinetic energy to pressure; no external power required.
18. Eco Snippets (2017). How To Make a Water Ram Off-Grid Water Pump. https://www.ecosnippets.com/alternative-energy/how-to-make-a-water-ram-off-grid-water-pump/, Source for: Ram pump operating on flow and weight of water alone; two moving parts.
19. Land To House Product Documentation. Hydraulic Ram Pump specifications. https://www.amazon.com/Hydraulic-Ram-Pump-Land-House/dp/B07235733W, Source for: Minimum 3-foot head pressure required; automatic continuous cycling.
20. Eaton / Boyd Corporation (2024). Thermosiphons: Passive Two-Phase Thermal Management Systems. https://www.boydcorp.com/thermal/two-phase-cooling/thermosiphons.html, Source for: Thermosiphons requiring no added electrical power; greater reliability than active cooling loops.
21. Ariat Technologies (2024). Introduction to Thermosiphon Systems. https://www.ariat-tech.com/blog/introduction-to-thermosiphon-systems-operation-and-applications.html, Source for: Continuous self-sustaining circulation driven by density differential and gravity.
22. Alliance Chemical (February 2025). AI GPU Liquid Cooling: Glycol Guide for Datacenters. https://alliancechemical.com/blogs/articles/ai-gpu-cooling-revolution, Source for: Liquid cooling approximately 25 times more efficient than air; 30-50% standard glycol concentration; propylene glycol preferred at server level.
23. Dober Performance Fluids (April 2026). Glycol for Direct-to-Chip Cooling in Data Centers. https://www.dober.com/performance-fluids/resources/glycol-data-center-cooling, Source for: OCP specifying propylene glycol as preferred server-side coolant; ASHRAE TC9.9 recommending CDU separation.
24. Data Center Dynamics (March 2026). You're as cold as ice: Antifreeze in liquid cooling. https://www.datacenterdynamics.com/en/analysis/youre-as-cold-as-ice-antifreeze-in-liquid-cooling/, Source for: Pure water having higher heat capacity and thermal conductivity than glycol solutions, the honest thermal tradeoff.
25. Mikros Technologies. Choosing a Liquid Coolant. https://www.mikrostechnologies.com/learn/trends-and-insights/coolants-for-data-center-liquid-cooling.html, Source for: Glycol requiring larger flow channels or increased heat exchanger surface area to match water-only cooling performance.
26. EAI Water (December 2025). How to Optimize Glycol Water Mixture for Maximum Efficiency. https://eaiwater.com/glycol-mixture/, Source for: 50% EG freezes at approximately -36C; 50% PG freezes at approximately -32C; concentrations above 60% reducing performance.
27. Sustainability Magazine (July 2025). How are Companies Pioneering Data Centre Zero Water Cooling? https://sustainabilitymag.com/news/how-are-companies-pioneering-data-centre-zero-water-cooling, Source for: Microsoft August 2024 closed-loop chip-level cooling saving 125 million liters per data center annually.
28. Network Installers / IEA (January 2026). Data Center Energy Consumption Statistics. https://thenetworkinstallers.com/blog/data-center-energy-consumption-statistics/, Source for: Cooling accounting for 30-40% of total facility energy use; average PUE of 1.56 industry-wide.
29. Electric Choice (2025-2026). U.S. Data Center Power Consumption Map by State. https://www.electricchoice.com/datacenters/, Source for: Virginia data centers consuming more than 1 in 4 kilowatt-hours of the state's total electricity.
30. USPTO Patent No. 8742611. Hydropower Generating System, Source for: Prior patent establishing technical basis of data center positioned above a hydropower generating module using descending cooling water to drive a turbine in a closed cycle.
Additional Sources & Citations
Privette et al. (2026). "Data Centers Water Footprint: The Need for More Transparency." AGU Advances, Feb. 27, 2026. agupubs.onlinelibrary.wiley.com
MOST Policy Initiative (2026). "Data Center Water Use." April 8, 2026. mostpolicyinitiative.org
Consumer Reports (2026). "AI Data Centers: Big Tech's Impact on Electric Bills, Water, and More." March 20, 2026. consumerreports.org
Lincoln Institute of Land Policy (2026). "Data Drain: The Land and Water Impacts of the AI Boom." Feb. 23, 2026. lincolninst.edu
Diaz-Marin, C. and Berquist, Z.J. (2025). "Flipping the Switch: Carbon-Negative and Water-Positive Data Centers Through Waste Heat Utilization." Energy & Environmental Science, 18: 8403–8413. Referenced via European Commission Environment, March 30, 2026. environment.ec.europa.eu
Microsoft (2024). "Sustainable by Design: Next-Generation Datacenters Consume Zero Water for Cooling." Dec. 9, 2024. microsoft.com
DataBank (2026). "Five Sustainability Trends That Will Define Data Centers in 2026." March 3, 2026. databank.com
Data Center Dynamics (2026). "Data Centers: The Ten Main Trends for 2026." datacenterdynamics.com
EESI (2026). "Data Center Power Demands Are Contributing to Higher Energy Bills." Feb. 24, 2026. eesi.org
Bloomberg (2025). "AI Data Centers Are Sending Power Bills Soaring." Sept. 29, 2025. bloomberg.com
CNN Business (2026). "Here's How AI Data Centers Affect the Electrical Grid." Jan. 18, 2026. cnn.com
World Resources Institute (2026). "From Energy Use to Air Quality, the Many Ways Data Centers Affect U.S. Communities." Feb. 17, 2026. wri.org
Amazon (2025). "Data Centers Don't Raise Your Electricity Bills: Study Confirms." Dec. 16, 2025. aboutamazon.com (Note: This study was commissioned by Amazon. Independent verification is advised.)
Rep. Alexandria Ocasio-Cortez (2025). "Ocasio-Cortez Secures Department of Energy Study on Impact of AI Data Centers on Americans' Electric Bills." Sept. 4, 2025. ocasio-cortez.house.gov
Rep. Kevin Mullin (2025). "Mullin Questions Data Center Impact on Residential Power Bills." Oct. 29, 2025. kevinmullin.house.gov
Foreign Policy Research Institute (2025). "Data Centers at Risk: The Fragile Core of American Power." Dec. 5, 2025. fpri.org
CoreSite (2026). "The Role of Data Centers in Powering 'Digital Everything.'" Jan. 8, 2026. coresite.com
Microsoft Datacenters. "What Is a Datacenter?" datacenters.microsoft.com
OPB / NPR (2025). "Data Centers Are Booming, But There Are Big Energy and Environmental Risks." Oct. 14, 2025. opb.org
Tao & Xu (2025). "Global Data Center Expansion and Human Health: A Call for Empirical Research." Eco and Environmental Health, May 27, 2025. pmc.ncbi.nlm.nih.gov
Yao & Xu (2025). "How Does Construction of the Healthcare Data Center Affect the Health of Older Adults?" Frontiers in Medicine, June 2, 2025. pmc.ncbi.nlm.nih.gov
Congress.gov / Library of Congress (2026). "Data Centers and Their Energy Consumption: Frequently Asked Questions." congress.gov
DataBank (2026). "The Truth About Data Centers: Why This Conversation Is Happening Now." databank.com
U.S. Department of Energy. Data Center Energy Projections (2023–2028). Referenced via multiple sources above.
International Energy Agency (IEA) (2025). Data Center and AI Energy Use Estimates. Referenced via multiple sources above.
All claims verifiable through citations above. No data was fabricated or estimated without source attribution. Originally conceived and freely released by Mylearningacademy.org | June 2026
CC0 1.0 Universal, No rights reserved, https://creativecommons.org/publicdomain/zero/1.0/
We are human and can make mistakes too. If you find something incorrect, feel free to point it out to us, and we will check it to see if your input is valid. We will not argue with any of you. Please be able to provide factual evidence, not a narrative.
Vaccines - What They Didn't Tell You
The Intramuscular Missing Link
Mapping the Gaps in Lifetime Cumulative Formaldehyde Exposure and Childhood Health Trends
Author/Source: My Learning Academy Research Hub
Date: May 2026
1. Executive Summary
Over the past several decades, public awareness and strict regulations have successfully reduced childhood exposure to major historical environmental hazards. Legacy pesticides like DDT have been banned, toxic chemicals in consumer plastics (like BPA) are actively avoided by parents, and dangerous chemical flame retardants have been phased out.
Paradoxically, during this exact same window, the rate of childhood cancer diagnoses has steadily risen.When a biological system is already processing a heavy daily background workload, adding an unfiltered, sharp, localized stressor could act as a tipping point.
This paper isolates the one major environmental and medical variable that has significantly increased in volume, frequency, and route of delivery over this timeline: the expanded childhood and adolescent routine immunization schedule.
Specifically, we investigate the institutional blind spot surrounding the cumulative lifetime impact of residual formaldehyde delivered via intramuscular injection.
2. Deconstructing the Science: The 2013 "Infant Study"
When public health agencies or medical websites want to reassure people that the trace amounts of formaldehyde in vaccines are perfectly safe, they almost always point to a single, famous study published in 2013 (known as the Mitkus study).
Most people reading public health factsheets assume that scientists took real, living human babies, gave them their routine shots, drew their blood, and measured how fast the formaldehyde cleared out, but that is not what happened.
The Missing Human Element
In that study, there was no physical human child. Instead, scientists built a mathematical computer simulation. Essentially, they used a software program designed to guess how a chemical might move through a generic body.The computer program was given specific rules. It was told the average weight, blood volume, and organ sizes of a 2-month-old and a 6-month-old baby.
It was programmed with a basic chemical rule: once a formaldehyde molecule enters a fluid like blood water, natural enzymes destroy half of it every 60 to 90 seconds (this is called its metabolic half-life).
The computer then simulated injecting a dose of 200 micrograms of formaldehyde into a digital "muscle pocket" and calculated how fast the virtual blood would wash it away and break it down. It then showed that because the chemical is highly water-soluble, it diffuses out of the muscle and is neutralized by blood enzymes within 30 minutes.
Naturally, the virtual blood levels stayed low, and regulators declared the trace amount safe.
Why a Computer Program Fails to See the Whole Picture
While a computer program is a useful calculator, it has major logical flaws when applied to a real, developing human life.
First, it monitors the wrong thing.
The software was only programmed to check if the entire blood supply of the baby would experience a massive, dangerous spike. It completely ignored what happens to the real, living cells and nerve endings inside the actual muscle tissue where the needle went in during those 30 minutes, when the chemical is highly concentrated in one spot.
Second, it creates a "Clean Slate" fallacy.
A computer program has no biological memory. As soon as a 30-minute simulation ends, the software completely resets to a perfect zero, but a real child's body does not have a reset button.
While the chemical molecule disappears quickly, the sharp chemical spike triggers a local cellular defense response, which causes tissue stress and activates immune cells (macrophages).
The Compounding Timeline:
In the software, each injection is an isolated mathematical event. In real life, a child undergoes this exact localized tissue stress sequence over and over again, at birth, 2 months, 4 months, 6 months, toddler milestones, early school years, adolescence, and potentially intensive military intake.
A computer program that deletes its own history every 30 minutes cannot measure the long-term, compounding impact of dozens of repeated tissue stress events over an 18-year lifecycle.
3. The Core Pattern Matrix
Intramuscular Injection vs. Dietary Ingestion
Traditional risk models frequently claim that because an apple or a pear naturally contains more micrograms of formaldehyde than a vaccine, injections are mathematically harmless.
This creates a false scientific equivalence by completely ignoring the physics of human anatomy and exposure routes.
Vector A: Oral Ingestion (Eaten)
When formaldehyde is eaten through whole foods, it encounters the body's highly evolved external filtration barriers.
THE BARRIER DELTA MATRIX
ROUTE 1: ORAL INGESTION (Eaten)
Food Consumption ➔ GI Tract Mucosa (Local ADH1/Enzymes) ➔ Portal Vein ➔ First-Pass Liver Filtration ➔ Systemic Blood
*Result: System protected by multiple metabolic checkpoints.*
The Gastrointestinal Shield:
The lining of the stomach and intestines are packed with local enzymes that immediately begin breaking down the compound.
First-Pass Liver Metabolism:
100% of the blood absorbing nutrients from the gut must travel directly through the portal vein straight into the liver. The liver acts as a massive security checkpoint, neutralizing the trace chemical before it ever reaches the heart, brain, or general systemic circulation.
Vector B: Intramuscular Injection (Injected)
When a compound is injected directly into deep skeletal muscle tissue, the body's primary protective shields are completely bypassed.
ROUTE 2: INTRAMUSCULAR ENTRY (Injected)
Skeletal Muscle Pocket ➔ Local Interstitial Fluid ➔ Direct Capillary/Lymph Diffusion ➔ Systemic Circulation
*Result: Protective barriers bypassed; local tissue must manage the entire gradient
Direct Tissue Pocketing:
The complete chemical mass is deposited directly into the local interstitial fluid of the muscle.
Bypassing the Security Gate:
The chemical diffuses across local capillary walls directly into systemic venous blood returning to the heart, entirely bypassing the portal vein and the protective first-pass filtration of the liver, which means the local tissue cells must manage the acute, high-intensity concentration gradient completely on their own.
4. The Regulatory Blind Spot and Circular Logic Loop
The National Toxicology Program, the International Agency for Research on Cancer (IARC), and the EPA officially classify formaldehyde as a known human carcinogen. However, this classification is based almost entirely on historical data tracking factory workers and embalmers who chronically inhaled gaseous formaldehyde over decades, leading to upper respiratory tract cancers.
There are no long-term occupational groups of humans being repeatedly injected with micro-doses of formaldehyde over decades, so regulatory bodies have simply assumed there is "no biological plausibility" for systemic cancer via the muscle pathway. This has created a self-reinforcing loop of circular logic within institutional science:
The Institutional Data Loop
├─────────────────────────────────────────┤
1. No longitudinal human studies are
ever funded or conducted.
│
▼
2. Therefore, zero empirical human data
exists on lifetime injection trends.
│
▼
3. Because no data exists, regulators
declare there is "no evidence" of
harm.
│
▼
4. Because they claim there is "no
evidence," they assume there is no
plausibility, so no studies are
needed.
├─────────────────────────────────────────┤
1. No longitudinal human studies are
ever funded or conducted.
│
▼
2. Therefore, zero empirical human data
exists on lifetime injection trends.
│
▼
3. Because no data exists, regulators
declare there is "no evidence" of
harm.
│
▼
4. Because they claim there is "no
evidence," they assume there is no
plausibility, so no studies are
needed.
Subsection 4.2: The Structural Framework of Pre-Clinical Non-Testing
Whenever institutional frameworks cite pre-clinical animal safety testing to justify ingredient security, they rely on a methodology that is fundamentally incapable of mapping a human lifecycle. International regulatory standards (WHO, 2005; EMA CHMP, 2010) dictate that animal "repeat-dose" safety trials compress multi-year human schedules into 2-week intervals, with mandatory tissue evaluation occurring a mere 48 to 72 hours after the final injection.
By design, no regulatory protocol requires or executes long-term, multi-month or multi-year tracking of living animal tissue to observe chronic cellular degradation, epigenetic modifications, or localized oncological trends following an intermittent injection schedule. High-dose, short-term animal termination models are fundamentally mismatched against the multi-decade tracking requested by this study.
5. Conclusion and Call for Further Empirical Research
The gradual, decades-long rise in childhood cancer rates cannot be mathematically explained by early diagnostic detection alone, nor can it be easily blamed on legacy household plastics and older pesticides that are actively decreasing in modern society.
A rigorous process of elimination points to a major, unstudied intersection: the long-term systemic and epigenetic impact of delivering repeated, localized, intramuscular chemical deposits directly into a developing biological system that is already processing its maximum natural metabolic workload.
We are not disputing the chemical rule that the free formaldehyde molecule is rapidly broken down by blood water enzymes.
We are, however, identifying a profound gap in empirical science. No longitudinal epidemiological study has ever tracked the relationship between repeated, lifetime intramuscular tissue stress events and long-term systemic health outcomes in living human populations.
Relying on a 30-minute computer simulation from 2013 to evaluate a lifetime of pediatric and adult medical protocols is a severe structural flaw in public health safety architecture. We may have identified a critical pattern link, but there is only one way to know for sure, and that is for institutional science to break out of its circular logic loop and fund true, empirical, long-term tracking of living human tissue.
Many scientists will often claim that "All chemicals classified as known carcinogens undergo standard 2-year rodent carcinogenicity bioassays. Therefore, formaldehyde has been tested."
However, there is the Exclusion Rule: According to the WHO and FDA non-clinical evaluation guidelines, formal 2-year carcinogenicity bioassays are explicitly not required for vaccines because vaccines are administered intermittently rather than continuously every single day for a lifetime (like a daily blood pressure pill or a cholesterol medication). Therefore, standard regulatory pharmacology states there is no biological rationale to fund or execute multi-year animal tracking for tumor development.
Section 5.2: The Solution
The Voluntary Retrospective Matched Model
To break the institutional dead-lock caused by traditional research rules, public health science must look to the existing population. A definitive safety study does not require scientists to withhold medical care from children. Millions of parents have already voluntarily chosen entirely vaccine-free paths for their families, creating an established, real-world control group.
We propose a multi-decade, voluntary health registry that utilizes Propensity Score Matching to align unvaccinated cohorts with vaccinated counterparts based on identical lifestyle baselines (including organic diet tracking, consumer plastic reduction, and geographic environmental quality). If a participant within either cohort develops an oncological or chronic health condition over their lifecycle, the study design mandates targeted histopathological tissue evaluations via biopsy or autopsy. Pathologists will microscopically scan local muscle sites and adjacent organ systems for long-term indicators of chronic cellular stress, persistent macrophage infiltration, and localized tissue fibrosis. By utilizing an existing, voluntary population, this model side-steps traditional ethical barriers while providing the empirical human tissue data that predictive computer simulations/animal studies cannot replicate.
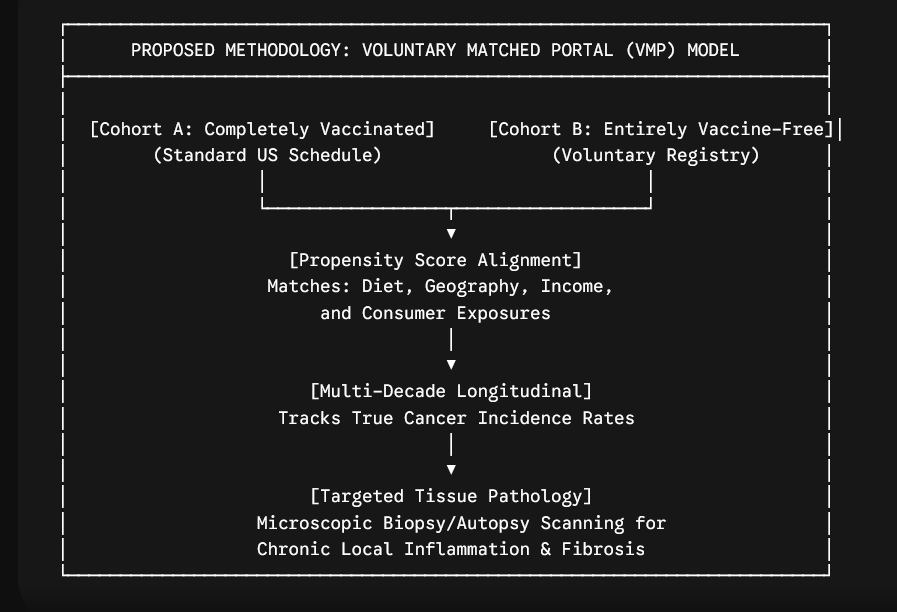
6. Comprehensive Technical References
Peer-Reviewed Literature & Computer Modeling
Peer-Reviewed Literature & Computer Modeling
Mitkus study (2013): Mitkus, R. J., Hess, M. A., & Schwartz, S. L. (2013). Pharmacokinetic modeling as an approach to assessing the safety of residual formaldehyde in infant vaccines. Vaccine, 31(25), 2738–2743.
Link: https://pubmed.ncbi.nlm.nih.gov/23583892/
Epidemiological Data & Cancer Registries
National Cancer Institute (NCI) SEER Explorer: Surveillance, Epidemiology, and End Results (SEER) Program Cancer Statistics.
Link: https://seer.cancer.gov/statistics-network/explorer/
Journal of the National Cancer Institute (JNCI) Trends: Racial and ethnic and socioeconomic disparities in childhood cancer incidence trends in the United States, 2000-2019.
Link: https://academic.oup.com/jnci/article/115/12/1576/7235569
Official Carcinogen Classifications
IARC Monograph 88: International Agency for Research on Cancer (2006). Formaldehyde, 2-Butoxyethanol and 1-tert-Butoxypropan-2-ol. Evaluation of Carcinogenic Risks to Humans.
Link: https://www.ncbi.nlm.nih.gov/books/NBK326468/
National Toxicology Program (NTP) Listings: Report on Carcinogens, Twelfth Edition. U.S. Department of Health and Human Services.
Link: https://ntp.niehs.nih.gov/
Environmental Assessment Profiles
ATSDR Toxicology Index: Agency for Toxic Substances and Disease Registry. Toxicological Profile for Polybrominated Diphenyl Ethers (PBDEs).
Link: https://www.atsdr.cdc.gov/toxprofiles/
EPA Environmental Guidance Databases: United States Environmental Protection Agency Core Risk Assessments.
Link: https://www.epa.gov/
Public Health Explanations
CHOP Vaccine Education Center Documentation: The Vaccine Education Center at the Children's Hospital of Philadelphia Information Sheet on Formaldehyde.
Link: https://www.chop.edu/vaccine-education-center/vaccine-safety/vaccine-ingredients/formaldehyde
Manufacturer Source Documentation
FDA Product Approvals Index: Full structural data, excipient limits, and individual manufacturer package inserts (such as GSK's Infanrix, Sanofi's Daptacel, or MCM's Vaxelis) can be searched and cross-referenced here:
Link: https://www.fda.gov/vaccines-blood-biologics/vaccines